Image 1: With hemorrhage washed away, lacerations are seen radiating from the liver, vaguely localized to the inferior border of the right lobe.
Question: What sequelae is our patient most at risk for in the immediate period following this liver injury?
Question: Generally, how at risk is the liver to traumatic abdominal injury?
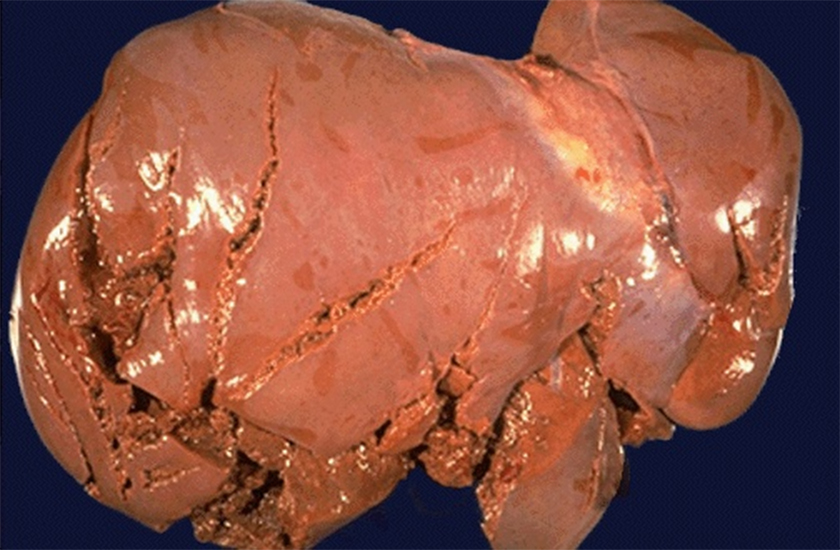
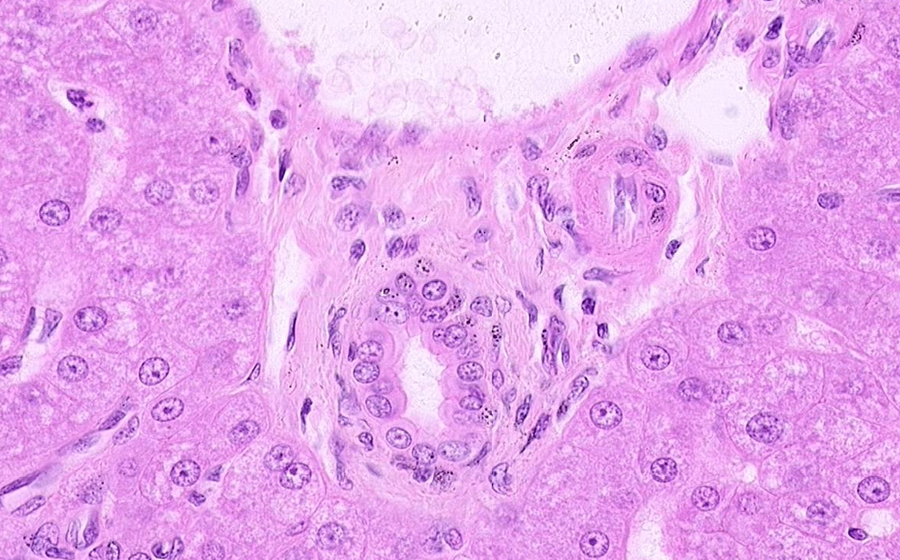
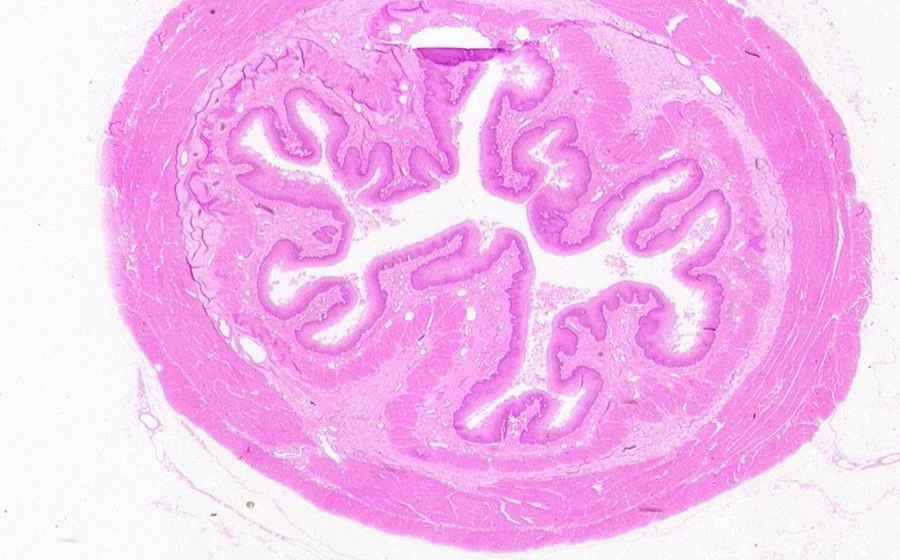
Image 2: A 3.5 cm mass was found in the descending colon upon longitudinally opening the bowel. The mass is typical of a pedunculated adenomatous polyp. The smooth, bosselated, cerebriform surface is hemorrhagic, and the mass is attached to the mucosal aspect by a stalk (peduncle). Colon polyps can also be grossly sessile, defined by the absence of a stalk and with the lesion appearing to sit directly on the mucosal surface.
Question: What gross qualities of this adenomatous polyp make it amenable to clinical surveillance?
Question: Contrast the gross features of this polyp that suggest it may be either benign or malignant?

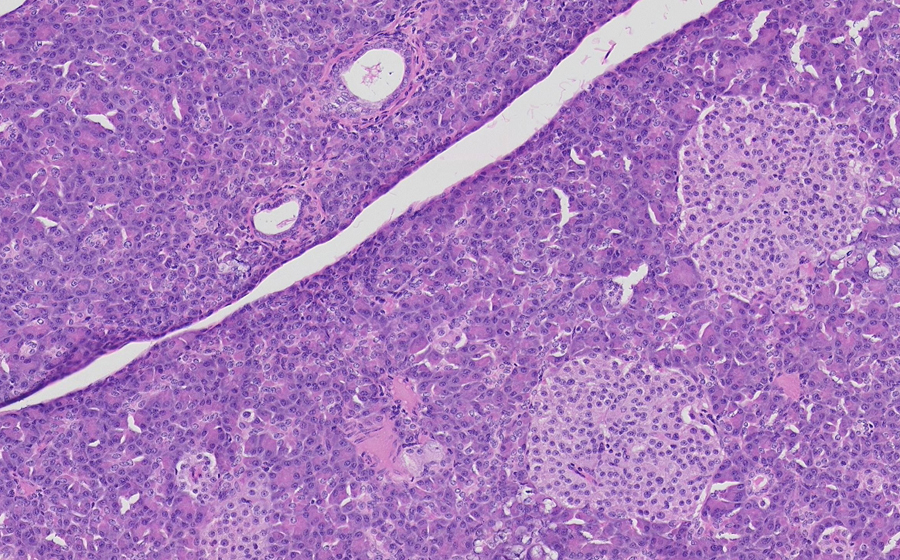
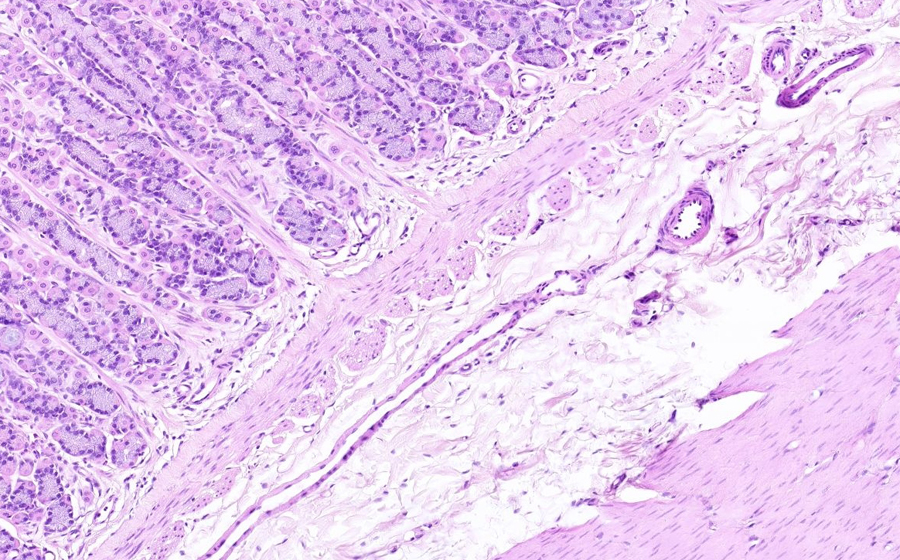
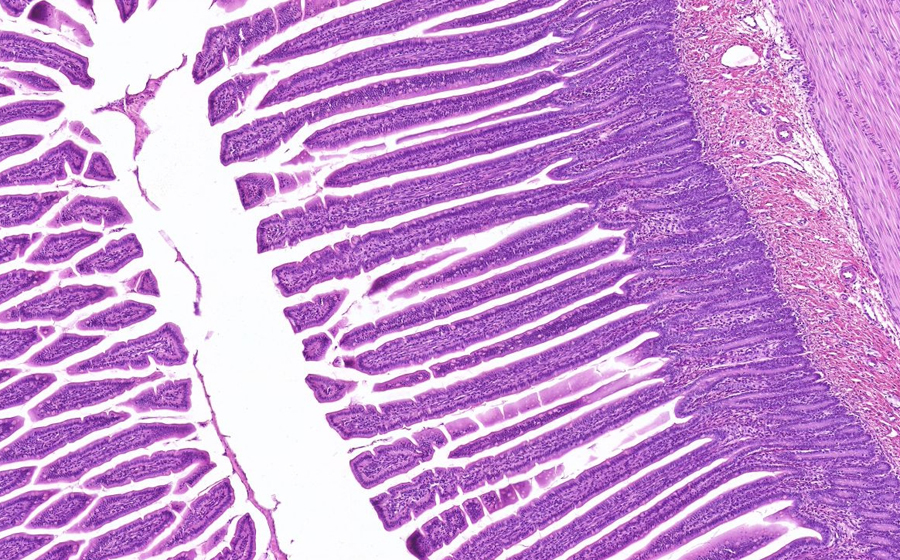
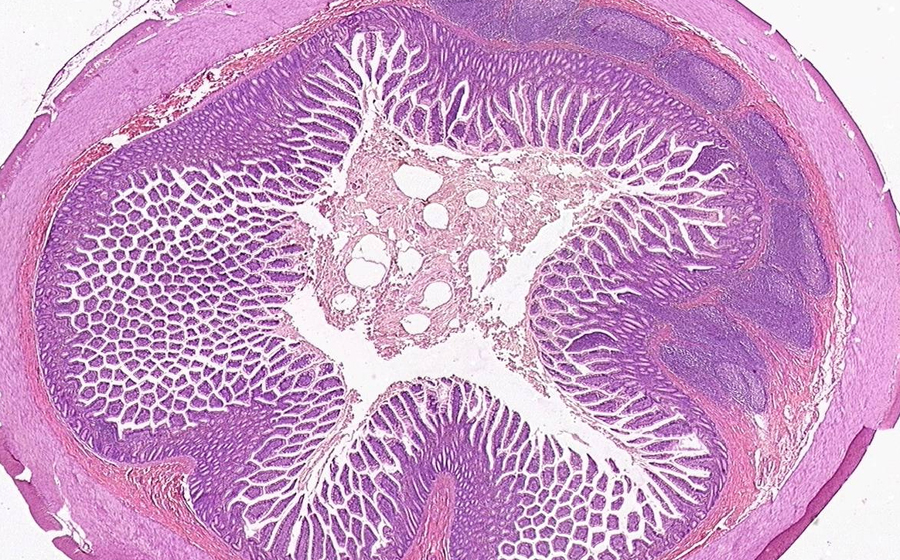
Image 3 (virtual): This slide is a representative section through the adenomatous colon polyp. On the right is a strip of normal colonic mucosa and superficial submucosa that transitions into the adenomatous polyp. At this low power, the pedunculated nature of the polyp is obvious, and the stalk is evident as a portion of submucosa that has been 'pulled up' into the expanding, mucosally-oriented neoplasm. Even at this power, glandular shapes formed by the neoplasm can be seen as more elongated and complex, and the glandular proliferation is more hyperchromatic than the epithelium that surrounds it.
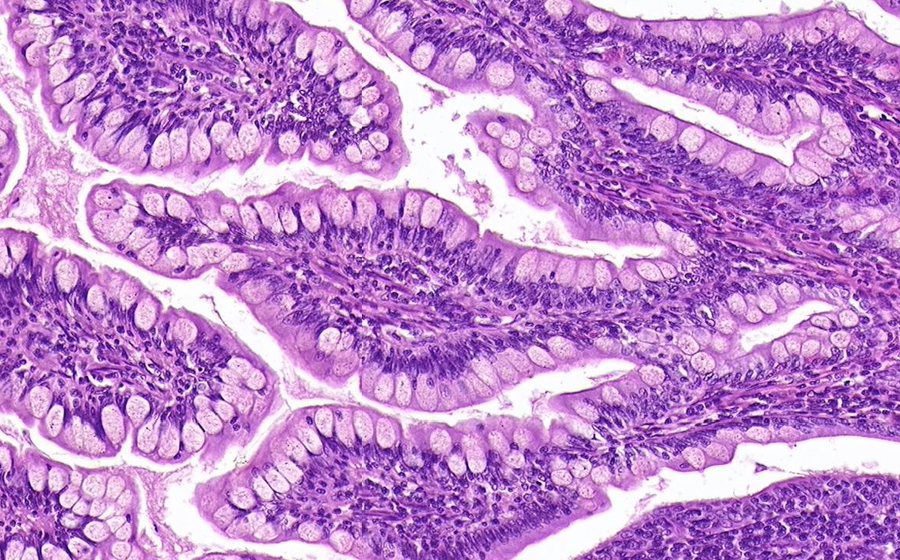
At high power, the glandular proliferation is replacing the mucosal surface, and the lamina propria appears less prominent as the neoplastic glands become crowded in some fields. Focus on a high power view of the neoplastic proliferation adjacent to normal colonic glands. While Goblet cells and absorptive cells are readily apparent in the normal field, these specializations appear lost in the neoplastic proliferation. The neoplastic glands show nuclear hyperchromasia with coarse chromatin, cellular stratification (the cells appear to 'pile up' on one another), and increased mitotic activity, including at the luminal surface. These features of dysplasia define an adenomatous polyp and indicate that the acquisition of mutations has occurred over time.
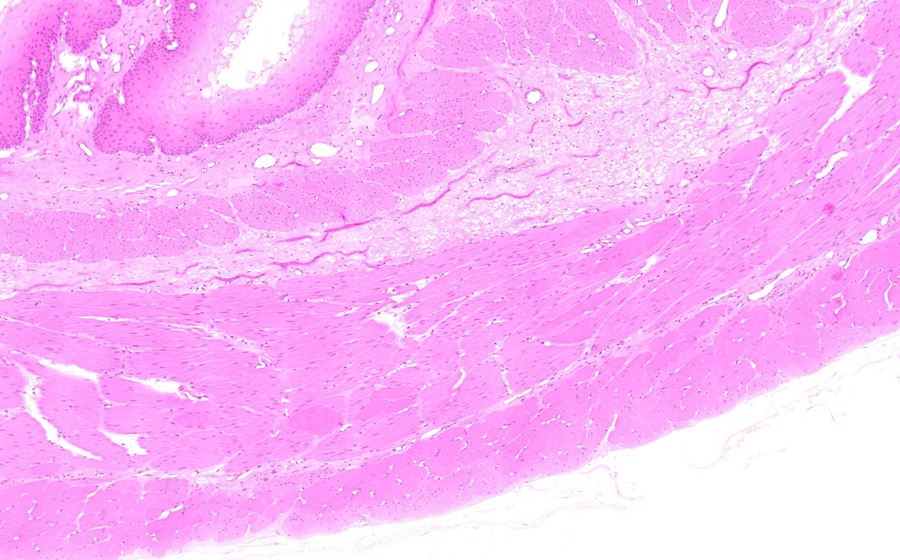
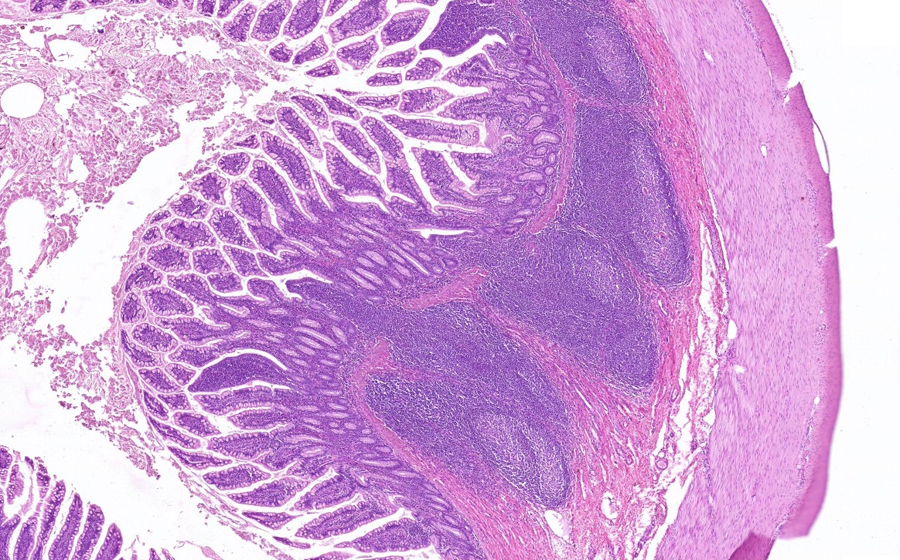
Now examine the distal-most stalk area/base of the polyp at medium-high magnification. Muscularis mucosae is present underneath the normal mucosa on either side; follow the muscularis mucosae from one normal side as it tracks toward the neoplastic proliferation. At some point, on both sides of the stalk, the muscularis mucosae is no longer apparent, and neoplastic glands are present instead. On the left side of the stalk, neoplastic glands are found directly under the intact muscularis mucosae, and are also in continuity with the primary neoplastic proliferation.
Question: What process is occurring in this neoplastic polyp at its base?
Question: What is your definitive diagnosis for the collective pathology on this slide?