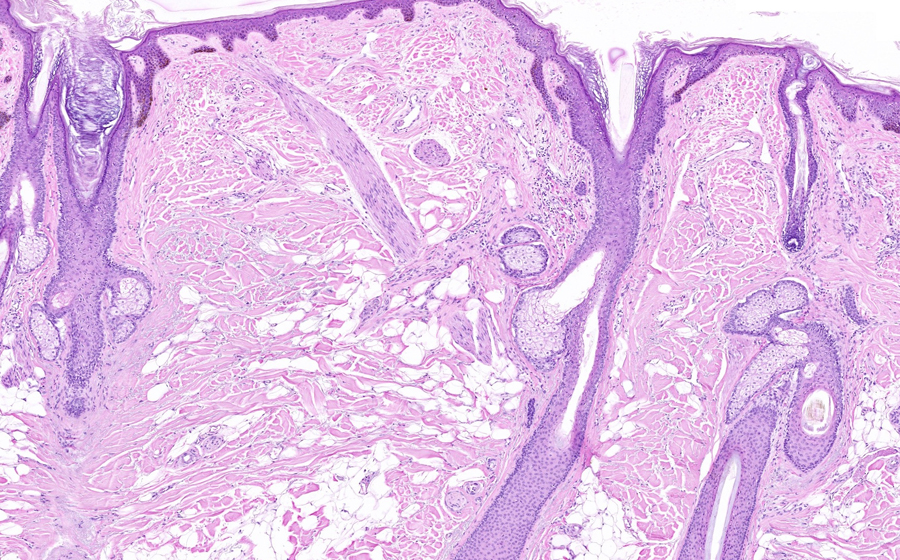
Image 1: Multiple acrochorda (singular: acrochordon; AKA: skin tag, fibroepithelial polyp, soft fibroma, squamous papillloma), up to 0.5 cm in size, are found on the patient's shoulder. These lesions are pedunculated and soft, covered by slightly hyperpigmented epidermis. Acrochorda are more typically seen in the middle and late ages of life, arising more likely in the intertriginous areas.
Question: How do the acrochorda in our patient differ from the more typical clinical presentation?

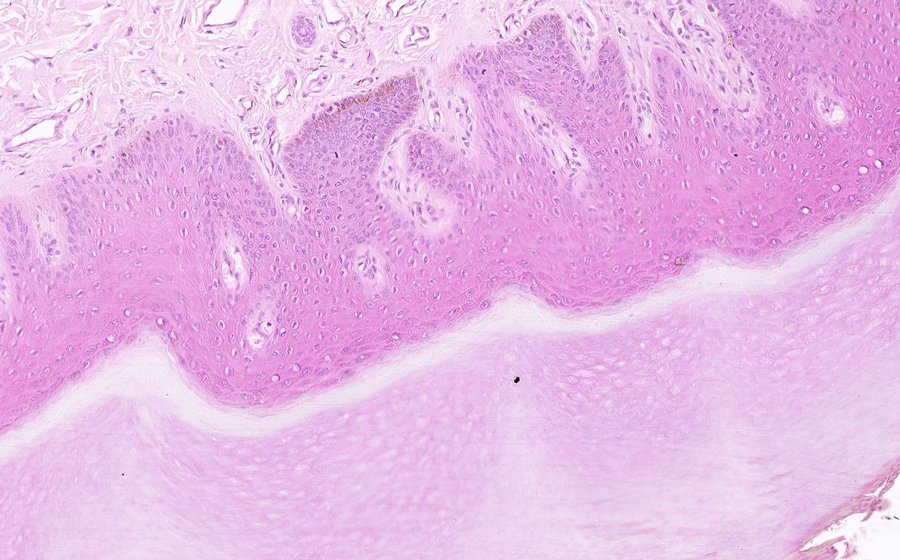
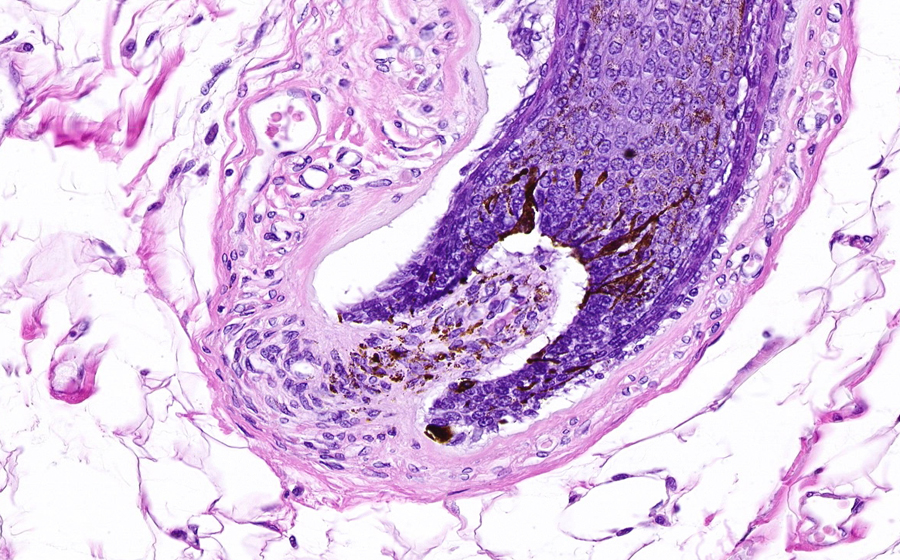
Image 2: From low power, a papillomatous portion of epidermis can be seen, and represents the removal of a single acrochordon. The base of the excision is at the uppermost portion of the section, appearing as interrupted and fragmented epidermis. The papillary nature of these benign neoplasms is evident in their growth as finger-like projections filled with fibrovascular stromal tissue. Some of the fibrovascular stroma is absent on the left half of the specimen, and this is an artifact of tissue processing.
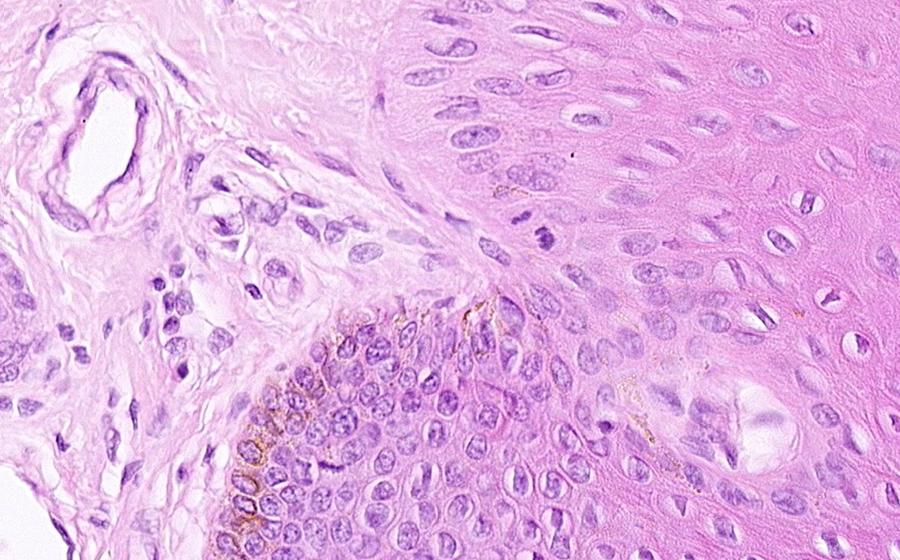
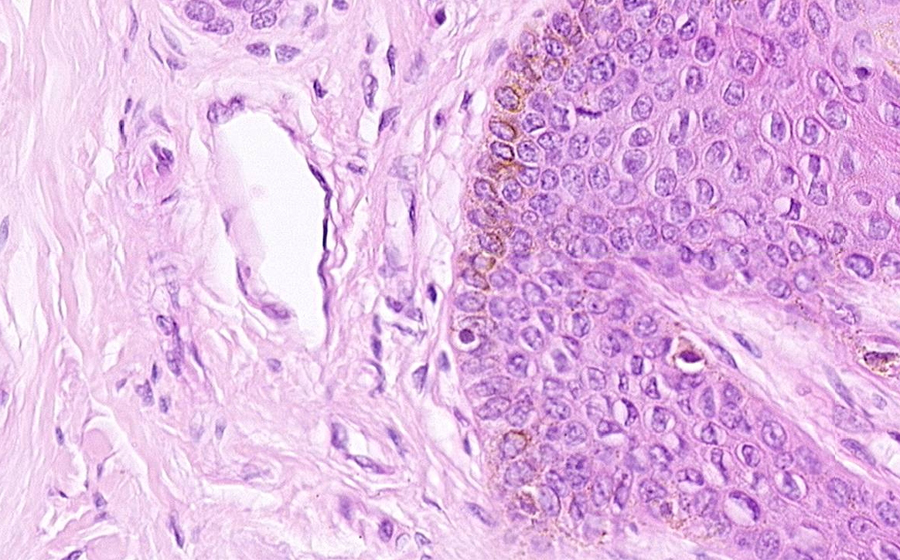
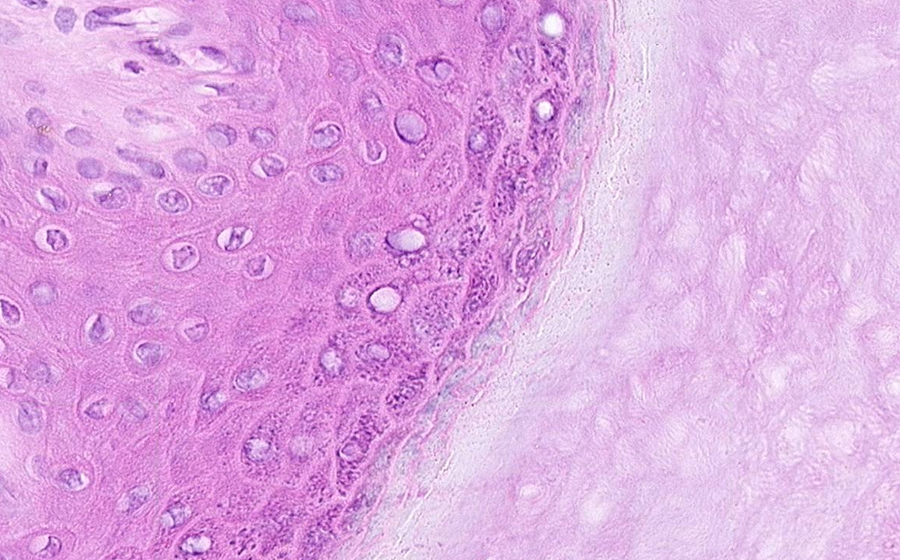
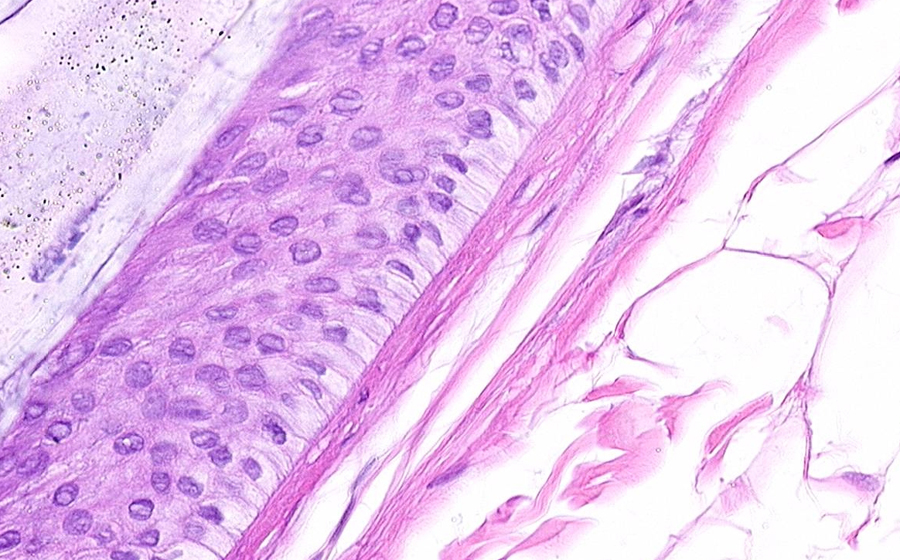
From high power, the epidermis is undergoing mild-moderate squamous hyperplasia (acanthosis), and is covered by focally prominent, basket-weave-type keratin. All layers of the epidermis can be identified, and no cytologic atypia is demonstrated by the keratinocytes. The eosinophilic basement membrane is also unremarkable and underlies the entire epidermis. The fibrovascular stroma consists of neoplasic expansion/elaboration of superficial papillary dermis. Loosely arranged collagen fibers, capillaries, and extracellular matrix predominate in the superficial dermis. As in normal integument, the fingerlike papillae of the superficial papillary dermis both interdigitate with, and help anchor, the dermis to the epidermis; this relationship can be appreciated in stretches of this neoplasm.
Question: If this neoplasm was a malignancy of dermal or epidermal cells, how might one expect the basement membrane to appear?
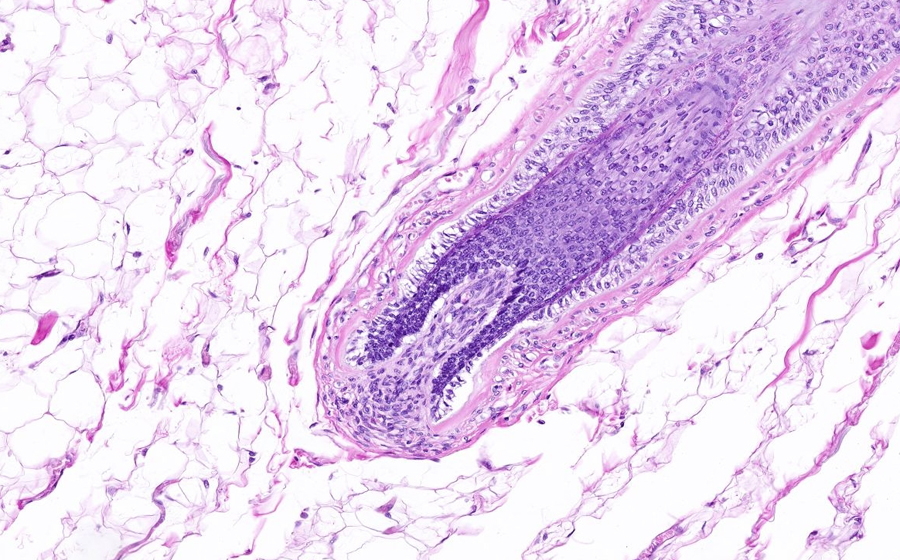
Image 3: This section is from the patient's back tattoo. From low power, dense eosinophilic dermal collagen predominates, and is covered by a thin and unremarkable epidermis. A portion of subcutis (subcutaneous adiopse tissue) is present at the base of section. Black coloration can vaguely be seen in the mid and upper dermis.
Question: How does this low power image differ from that expected of a section of normal scalp?
At higher power, the epidermis appears unremarkable and contains a thin layer of dense keratin. The superficial papillary dermis is relatively flat with a lack of prominent finger-like papillae (particularly evident at medium power). Few adnexal structures, including hair follicles or sebaceous glands, are evident.
Question: How would these features differ from a histologic section through the patient's palm?
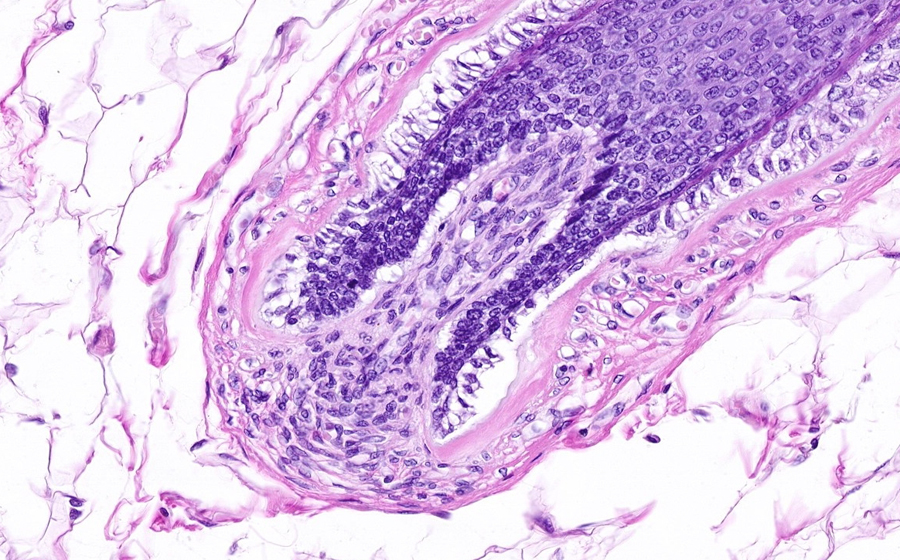
At high power, dense collagen bundles can be seen throughout the reticular dermis, a feature normal to this region of skin. Accumulated black pigment is present in an irregularly distributed pattern that is most prominent in the reticular dermis. This is the tattoo pigment that will reside in dermal macrophages over the course of the patient's life. Very small foci of black pigment may be appreciated as somewhat (macrophage) cell-contained, but this vague distinction is lost in the larger foci. Note the lack of other inflammatory cells or tissue reaction in or around the tattoo pigment. These few histologic features are typical of the body's response to handling certain non-melanocytic pigments (like tattoo ink), and are arguably somewhat underwhelming when compared to potential surface coloration or design.