Image 1: Lacerations of various size and depth are found over the occiput, and are associated with a large contusion of the region. This is the site of impact of the primary injury , also know as the coup (French: "blow") injury in forensic pathology, neurology, and medicolegal terminology.
Question: How is a laceration generally defined?
Question: What areas of the body are more prone to lacerations?

Images 2a and 2b: The surface of the patient's brain is depicted on the left. The frontal lobe appears distorted and has abundant, adherent hemorrhage. Hemorrhage can be seen tracking over the surface of the temporal lobes. This frontal lobe cortex pathology is the contrecoup injury (French: "opposite to blow"). When the brain undergoes sudden deceleration, the cranium is impacted differently than the brain matter, in that the cranium comes to an immediate stop. However, the brain matter can continue to move, due to inertia and the fluidic CSF that surrounds it, and sometimes rebounds forcefully against the cranium opposite to the impact.
Question: In the schematic, name the coup and contrecoup injured regions of the brain.
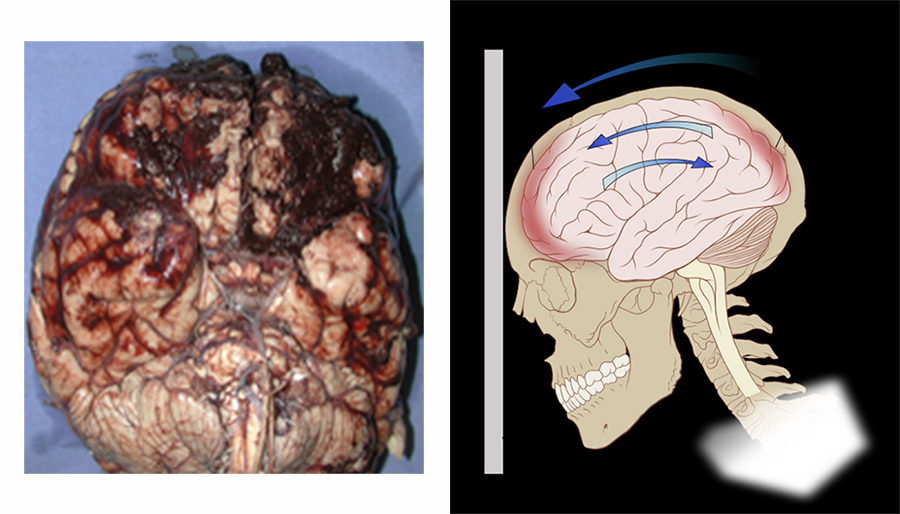
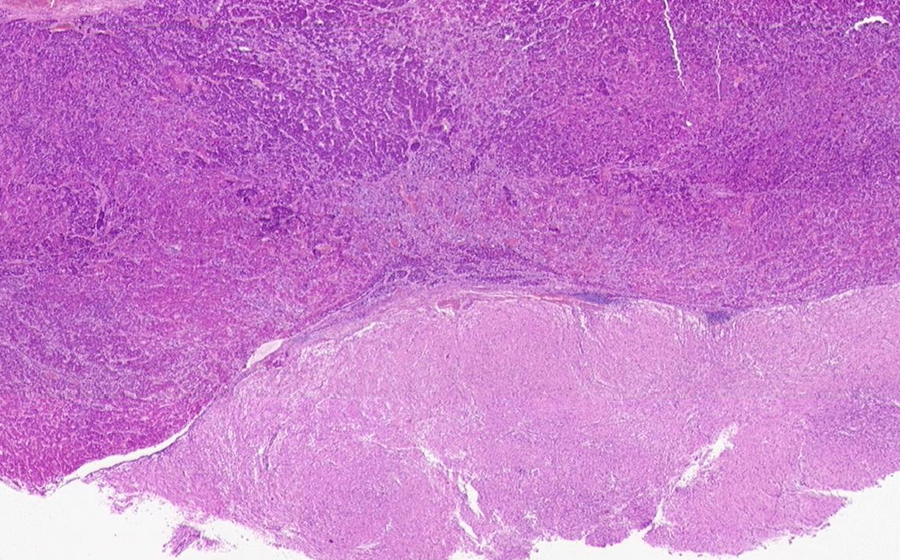
Image 3: With the brain removed, a circumscribed, 4.0 cm mass is seen protruding from the the sella turcica and into the suprasellar region. The mass is soft and well-circumscribed.
Question: Which anatomic structures can be affected by a mass in this region?
Question: What clinical symptoms can result from this mass effect?
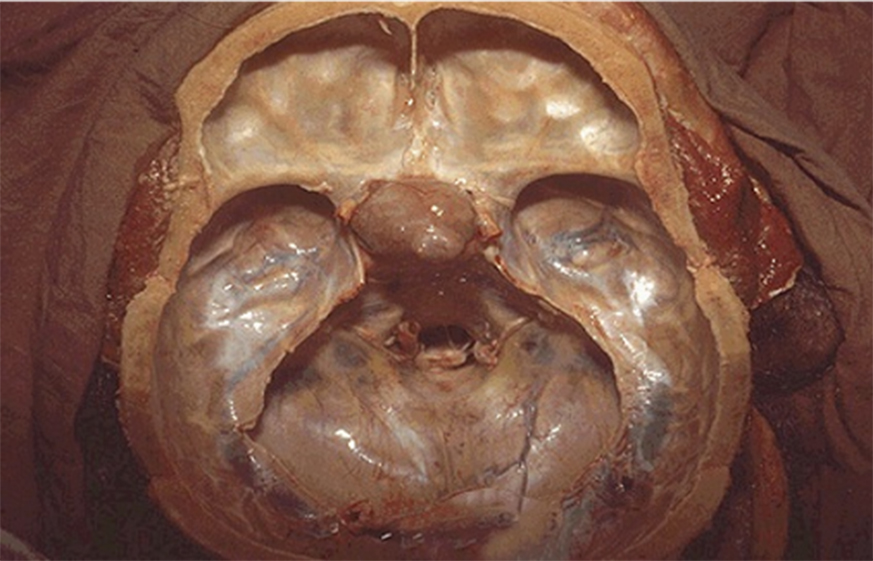
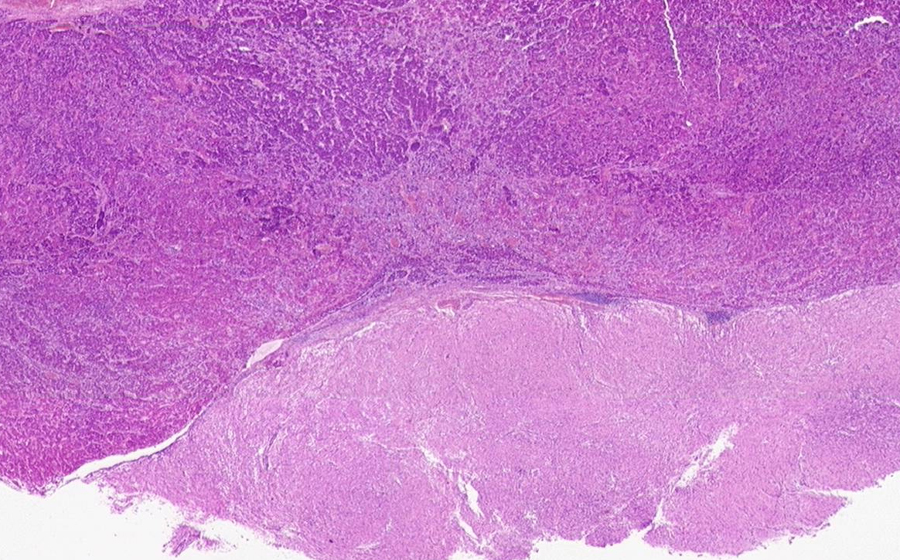
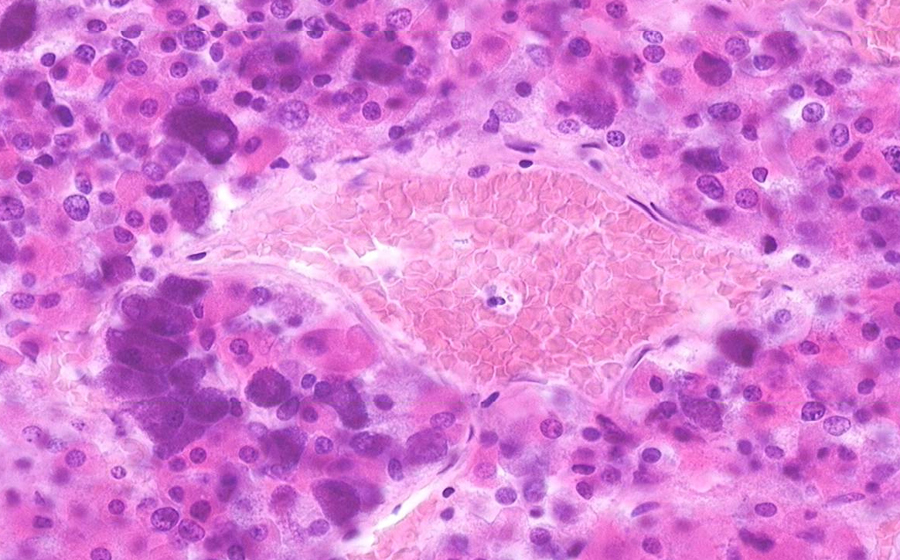
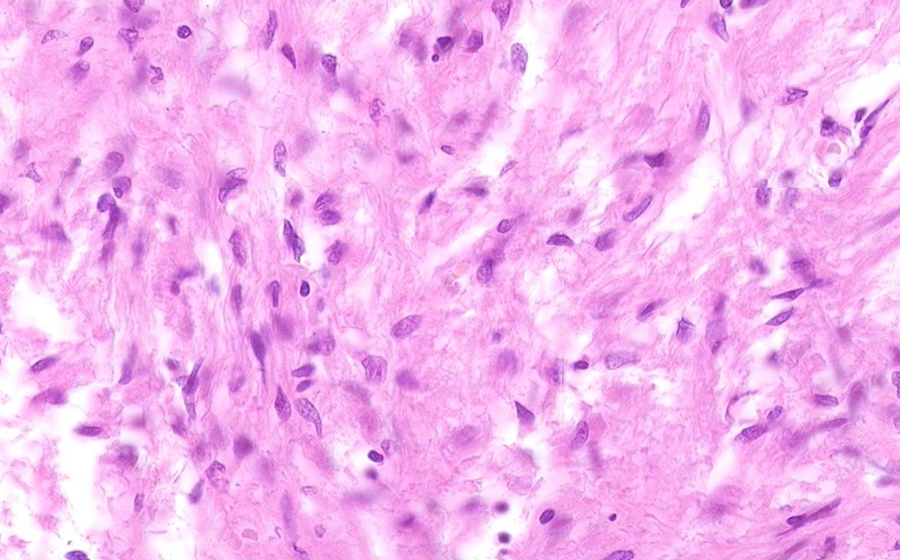
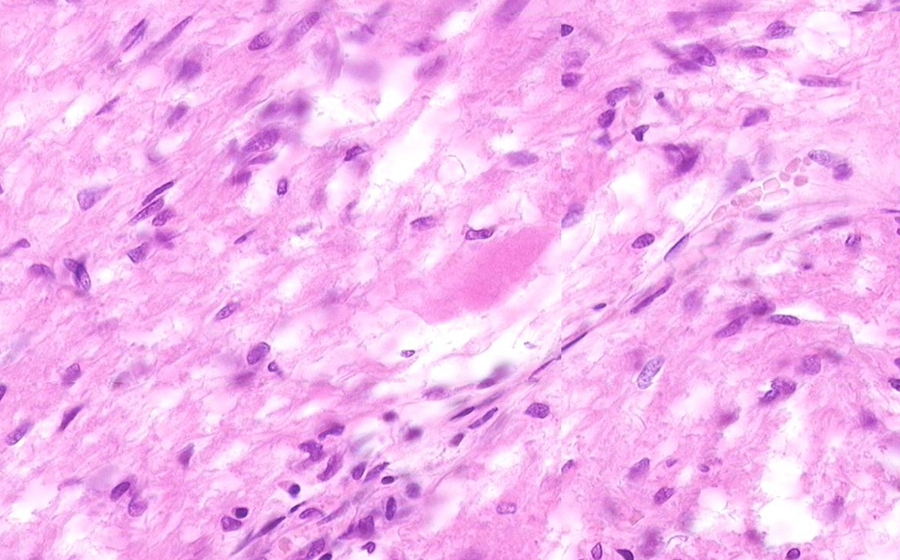
Image 4: This histologic section is taken from the mass in the sella turcica. From low power, a solid proliferation of cells is evident.
Question: Can any normal tissue be recognized on the slide at low power?
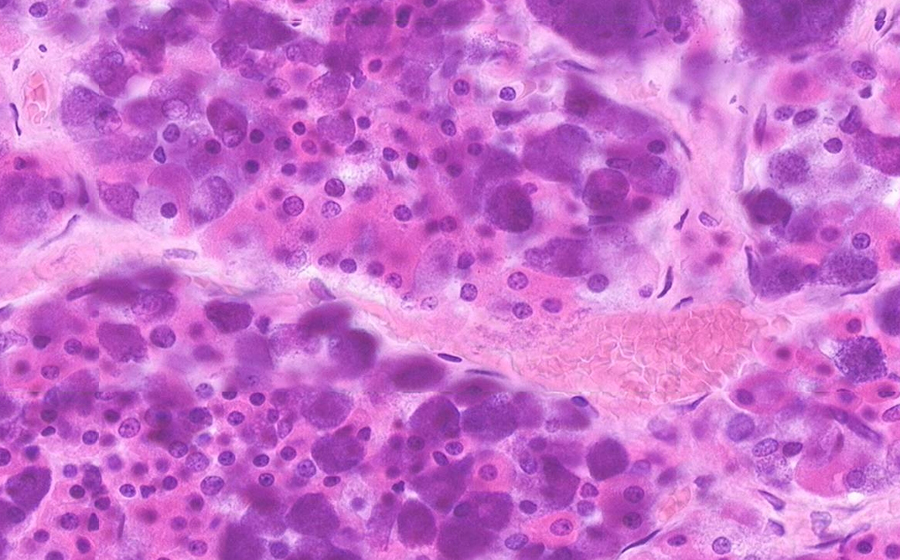
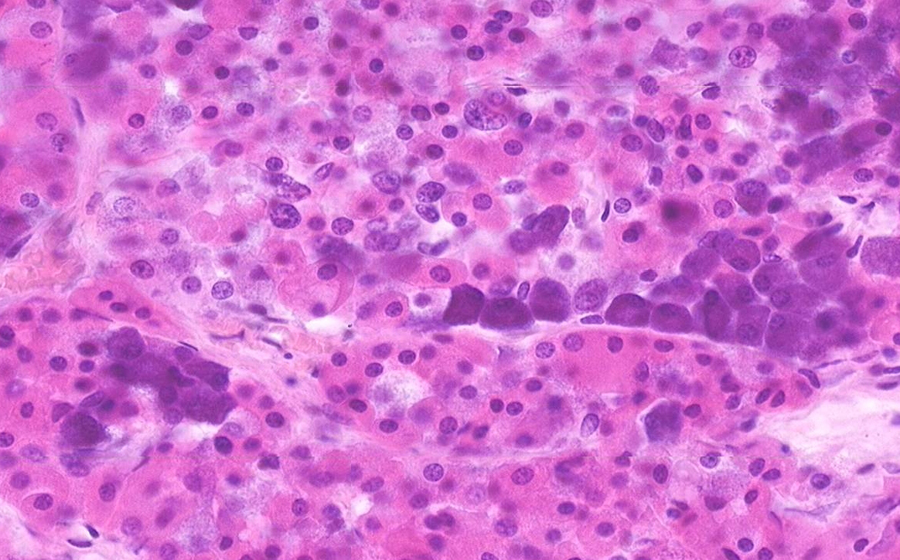
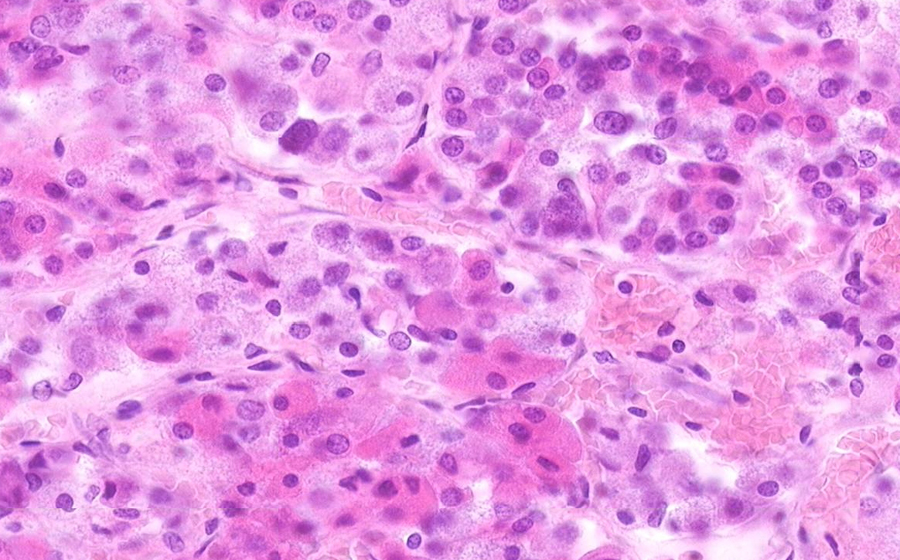
On high power, polygonal cells are arranged in small nests or cords, surrounded by a delicate network of supportive fibers and capillaries. The nuclear and cytoplasmic features of the cells are fairly uniform and consistent across all visual fields, demonstrating cellular monomorphism; no significant anaplasia or mitotic activity is appreciated. Nucleoli are not prominent, and nuclear chromatin appears relatively open. While there may be some nuclear hyperchromasia, this is likely due to the thickness of the tissue section, creating a visual artifact. Scan the slide and appreciate the visual monotony.
Question: Would the predominate cell type be described as acidophilic, basophilic, or chromophobic?
Question: What cell types from this region may demonstrate this histology?
Question: Is this sampled tissue normal or neoplastic? Benign or malignant?