
Image 1: Cut surfaces of the liver are diffusely uniform and reveal an alternating red-brown and light brown stippled pattern.
Question: What is the name and etiology of this gross liver change?
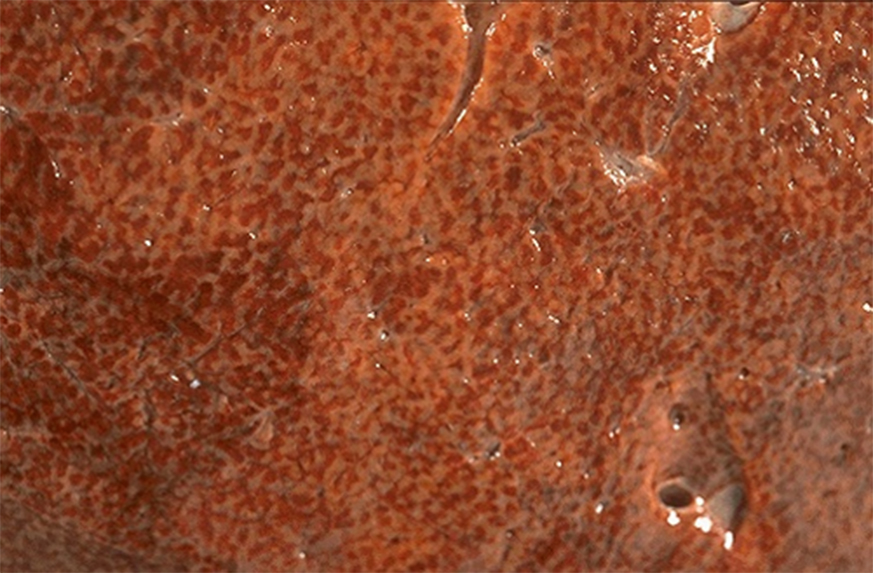
Image 2 (virtual): Right heart failure leading to (backflow/downstream) congestion causes liver pathobiology.
Q: Describe the major venous anatomy from the hepatic central veins to the right atria.
At low power, this slide shows a mixture of basophilic, eosinophilic, and pale areas. Eosinophilia is being imparted by congestion, as right heart failure precipitates central vein congestion, expansion and backflow 'hemorrhage' into the hepatic sinusoids - the process of central passive congestion.
At high power, and around the mostly unremarkable portal triads, basophilic hepatocytes contain microvesicular steatosis - round lipid droplets that don't displace or distort the nucleus. Central veins are difficult to identify in this slide, and are located somewhere in the middle of the hemorrhagic areas. Note macrovesicular steatosis affecting the hepatocytes (and markedly distorting their nuclei) in this area, likely due to on-going cellular injury in this region, and resembling the circular space formed by the contour of a central vein, further making the latter difficult to identify. These hepatocytes are less well-defined and somewhat shrunken in size, as centrilobular congestion fills central veins due to outflow obstruction, appears on a two-dimensional slide as 'hemorrhage' into sinusoidal spaces, and imparts pressure against the hepatic parenchyma. These zone 3 (centrilobular) hepatocytes, in the setting of right heart failure, are at risk for hypoxia due to several reasons: they are receiving the least amount of highly oxygenated blood normally, which is exacerbated by states of poor perfusion (such as in left heart failure), and combined with concomitant pressure phenomena from central vein congestion, all of which can lead to centrilobular hepatocyte necrosis. Try to identify the eosinophilic ghost cells of necrotic hepatocytes in and around the congested centrilobular regions.
Image 3: Upon entering the abdominal cavity, dusky loops of small intestine are evident, with some segments appearing almost black. The more affected small intestine on the right shows scant stringy material on the serosal surface.
Question: Given these gross features, what pathologic process must have occurred?

Image 4: The large colon also shows a 13.0 cm segment of dusky serosa involving the right mid colon. Upon opening the colon, abundant luminal blood and blood clot is present. Following light washing away of the luminal contents, the necrotic mucosa can be visualized.
Question: Given the large colon and small intestine gross features, what anatomical structure is most likely implicated in this process?

Image 5 (virtual): From low power, through this full-thickness section of the colon pathology at its transition with more grossly normal colon, the right half of the slide appears different than the left. While vascular congestion is more prominent on the left, mucosal and intramural hemorrhage predominate on the right. In addition, the mucosa shows a distinct change in appearance at about the midpoint of the slide. With magnification, on the extreme left, the normal histologic layers of the colon can be easily identified. Upon scanning over to the right though, these layers become more ill-defined.
Question: Identify the histologic layers of the colon on the extreme right of the slide.
The histology of necrosis is evident on the right half of the slide, and distinct boundaries or landmarks in the colon wall have become less clear. The full thickness of the colon is infiltrated by neutrophils, which can be seen extending onto the serosal surface, infiltrating the mucosa, and in all tissue planes in between. Although much of the epithelium is necrotic and sloughed off, some of the colonic glands are still vaguely present as eosinophilic, washed out appearing ghost cells. Submucosal vessels are difficult to identify and largely no longer intact, and hemorrhage is found extending throughout the tissue. Smooth muscle cells of the muscularis mucosa and the muscularis propria appear as curvilinear strips of degenerating and necrotic fibers surrounded by neutrophils and/or hemorrhage.
Question: What morphologic type(s) of necrosis are evident on the slide?
Question: Given the tubular nature of the colon, what is the distribution of necrosis called on the slide?
