
Leukemoid Reaction
- A blood picture showing marked leukocytosis, with a large number of immature WBC’s in circulation
- Similar to a "left shift," but with a more robust elevation, and of various WBC’s (not just neutrophils)
- WBC elevation may be large enough to make one consider (incorrectly) hematopoietic neoplasia
- General features/criteria:
- Elevated WBC count (> 25,000)
- Platelet count normal
- Toxic granules present/positive
- Spleen normal size
- Dohle bodies present
- Philadelphia chromosome negative/no cytogenetic abnormalities
- Elevated leukocyte alkaline phosphatase (LAP)
Causes of a leukemoid reaction
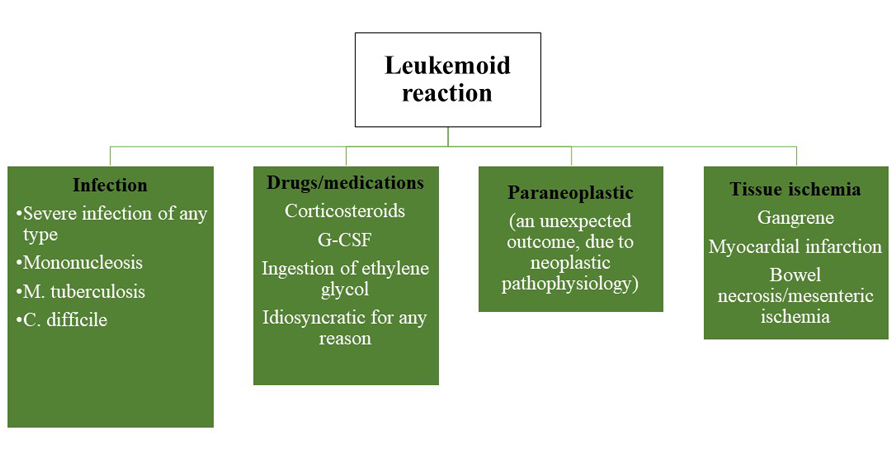
Schematic by Paul J Kowalski, MD, Michigan State University
Infectious Mononucleosis
- Classic presentation: fever, sore throat, lymphadenopathy, and (sometimes intense) fatigue; atypical presentations include only fatigue and/or lymphadenopathy
- Etiology: primary infection with EBV (Ebstein-Barr virus); CMV (cytomegalo-virus) can cause as well, although less commonly
- Pathogenesis: usually through direct oral contact (“kissing cousin” disease), viral infection of oropharyngeal squamous epithelial cells, and eventual spread to regional lymphoid tissue
-
Diagnosis:
- Finding atypical lymphocytes in the peripheral blood
- Positive heterophil reaction (Monospot test) for EBV
- Rising titers of antibodies specific for EBV antigens
- Epidemiology: ubiquitous, with most children-young adults infected, and > 90% of populations infected by 60 y/o.
End of Discussion
